


Επιλεγμένες Επιστημονικές Δημοσιεύσεις
Idiopathic True Aneurysms of the Brachial Artery: A Short Case Series and Scoping Review
M. Leonida, S. Papadoulas et al. J. Clin. Med. 2026,15,295. https://doi.org/10.3390/jcm15010295. Department of Vascular Surgery, University of Patras Medical School, Patras, Greece
Background: Brachial artery aneurysms are a rare entity occurring sporadically at all ages. Common causes are trauma, infection, connective tissue disorders, genetic syndromes, immunosuppression, and a history of arteriovenous vascular access. Pseudoaneurysms are
mainly of traumatic or iatrogenic origin. Idiopathic true brachial artery aneurysms are even
scarcer, attributed to inherited susceptibility for aneurysm formation or to atherosclerosis.
Due to the rarity of these aneurysms, we report our experience along with a current literature review.
Methods: A retrospective search was conducted in the Vascular Surgery Department database of a tertiary referral center for vascular surgery, covering procedures from January 1991 to October 2025. Patients were included if they had undergone idiopathic true brachial artery aneurysm repair. Clinical records, operative details, imaging studies, and follow-up data were reviewed. We additionally provide a literature review regarding clinical presentation,signs,pathophysiology, diagnosis, and treatment of these aneurysms.
Results: Amongst all procedures performed for aneurysmal repair, in the searched period, we identified three patients who met these criteria. All three underwent successful elective operations. Individual characteristics of the retrieved cases are reported.
Conclusions: The open repair of true idiopathic brachial artery aneurysms is a technically simple approach
that leads to satisfactory outcomes. Endovascular therapy is technically unfavorable in this
type of aneurysm.
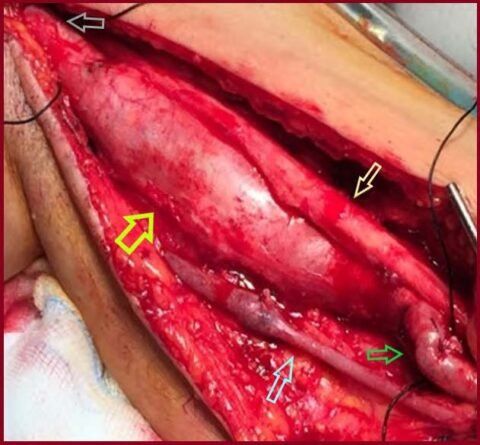
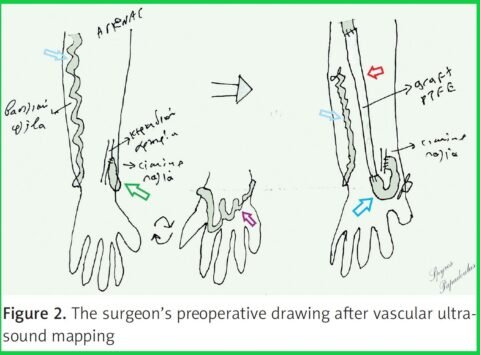
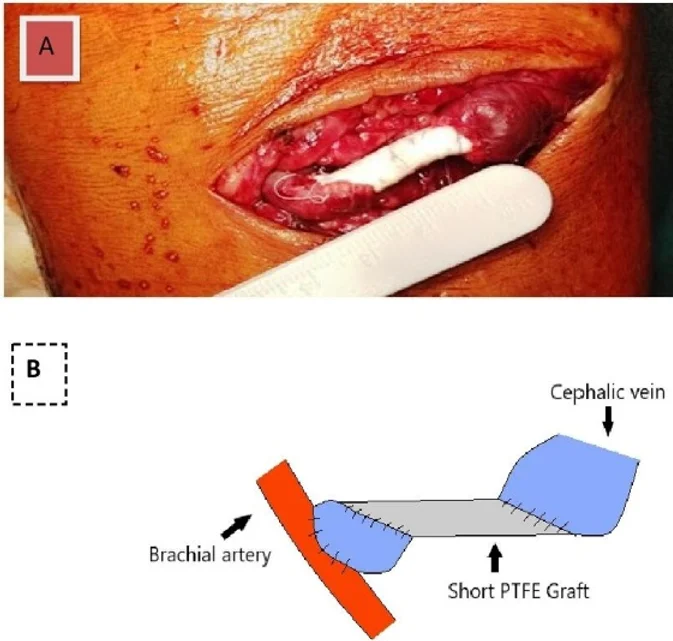
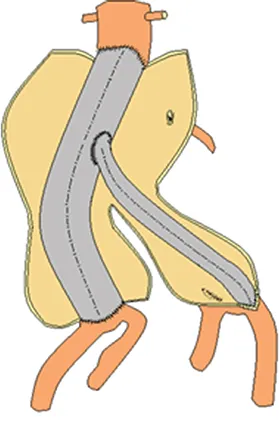
Maintaining functionality by graft interposition in a Brescia-Cimino arteriovenous fistula resembling an ulnar-basilic fistula
S. Papadoulas et al. Pol J Thorac and Cardiovasc Surg 2025; 22 (4): 299-301. DOI: https://doi.org/10.5114/kitp.2025.158043. Department of Vascular Surgery, University of Patras Medical School, Patras, Greece
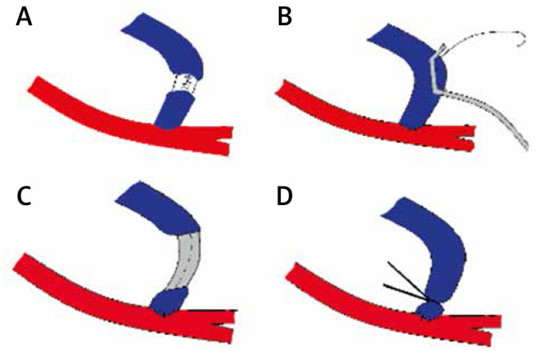
A 49-year-old female patient on chronic dialysis for the last 13 years was referred for a dysfunctional left side-to-side Brescia-Cimino fistula created in another institution, 14 years previously. She had a history of nephrectomy after a severe traumatic injury at the age of 16. Her medication included clopidogrel 75 mg o.d., omeprazole 20 mg o.d. and sevelamer carbonate 800 mg, 2 tbs t.i.d. The efferent cephalic vein was thrombosed, and cannulation was impossible via a serpentine and kinked basilic vein in the forearm. Hemodialysis was performed by a permanent tunneled catheter placed in the right jugular vein. After a color duplex ultrasound evaluation, forearm cephalic vein thrombosis was confirmed, but the fistula functioned via the patent afferent wrist cephalic vein. This vein was draining in the forearm basilic vein, through a dilated venous network at the dorsal aspect of the hand. The flow volume was 700 ml/min. Deep veins were patent. This anatomic venous configuration resembles the venous outflow of an ulnarbasilic vein (Figure 1). Preoperative percutaneous digital subtraction venography revealed normal patency of the upper arm cephalic, basilic, and central veins. The patient underwent interposition of a synthetic 4–7 mm graft
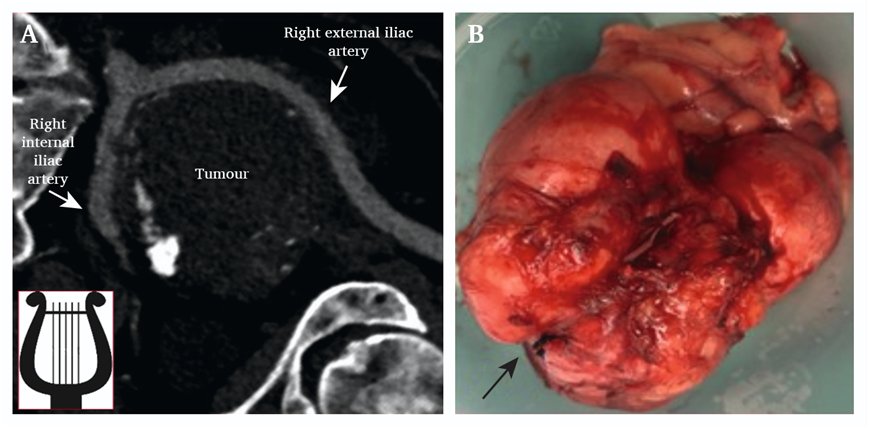
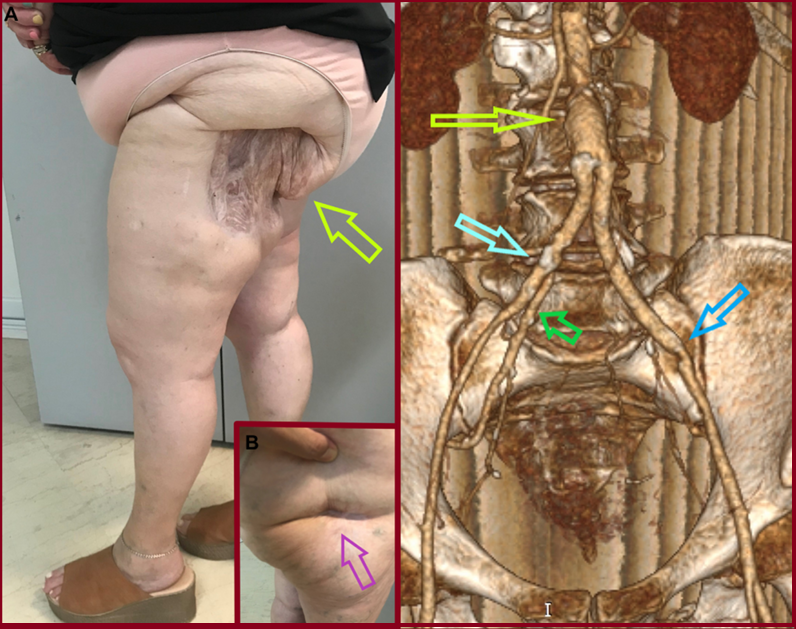
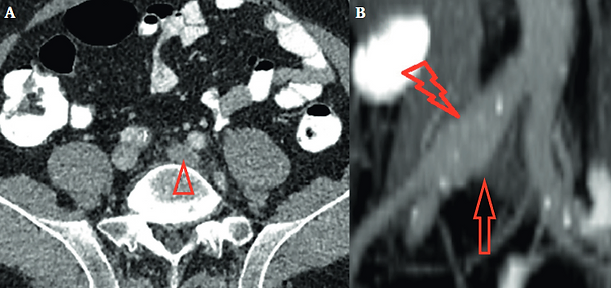
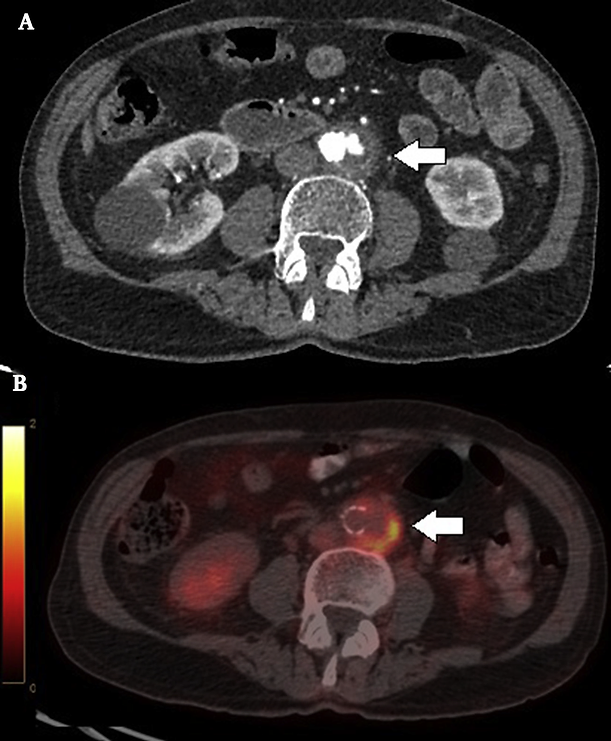
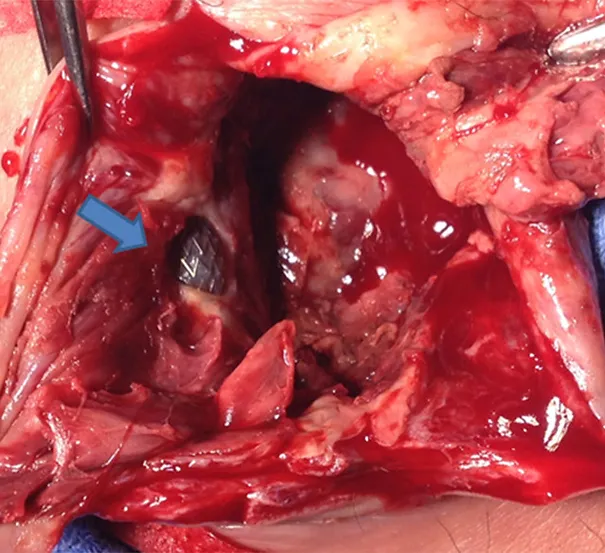
The Lyre Sign in Oncovascular Surgery
Spyros Papadoulas, Ioannis Maroulis. The Lyre Sign in Oncovascular Surgery. Eur J Vasc Endovasc Surg. 2025 Nov 27:S1078-5884(25)01182-7. doi: 10.1016/j.ejvs.2025.11.039. Epub ahead of print. PMID: 41317953.. Department of Vascular Surgery, University of Patras Medical School, Patras, Greece
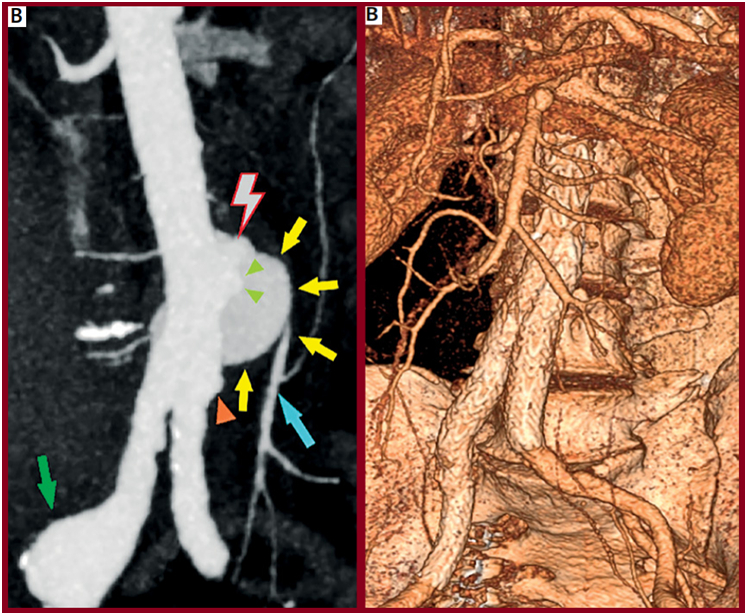
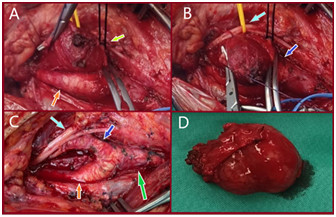
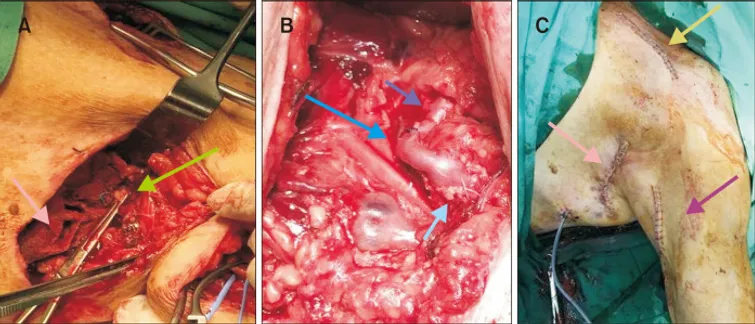
A 59 year old woman was admitted with a pelvic liposarcoma (without metastases) splaying the right external and internal iliac arteries, forming a reversed ‘Lyre sign’ (A). Through midline laparotomy, the common and external iliac arteries were looped, and the external iliac artery was freed from the tumour. The tumour was successfully resected (including local lymphadenectomy) along with the external iliac vein (B, black arrow), as it was infiltrated. Despite the use of compressive stockings and prophylactic low molecular weight heparin administration, the patient developed post-operative deep venous thrombosis, which was treated with rivaroxaban. Adjuvant chemoradiotherapy and radiotherapy is planned.
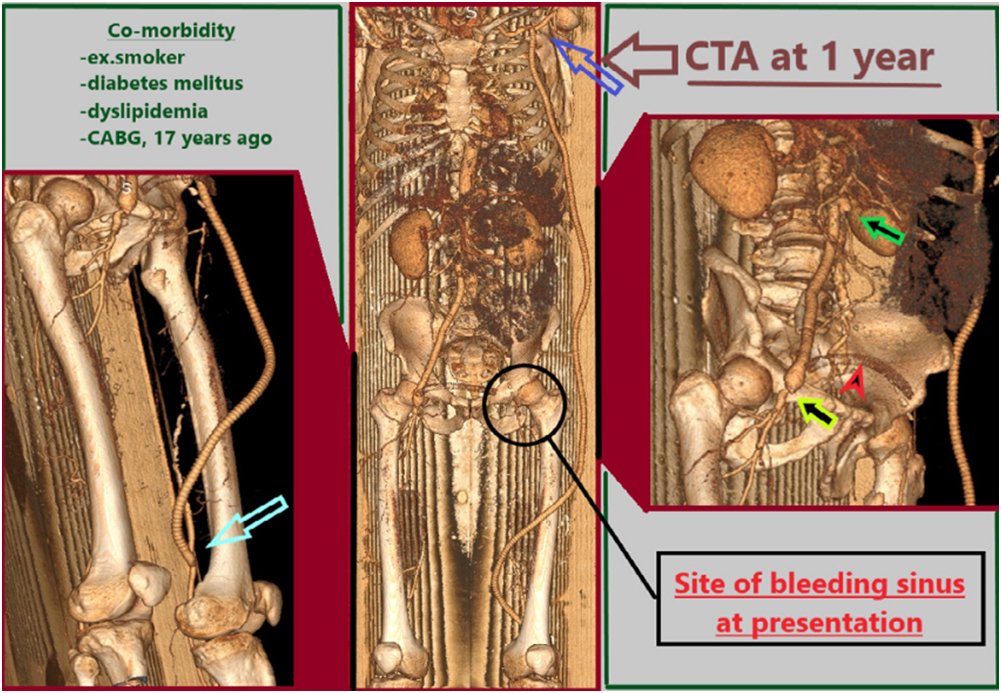
An urgent axillopopliteal bypass to treat a bleeding infected anastomotic groin pseudoaneurysm
M. Stathopoulou, S. Papadoulas et al. Hellenic Journal of Vascular and Endovascular Surgery | Volume 7 – Issue 1 – 2025. Department of Vascular Surgery, University of Patras Medical School, Patras, Greece
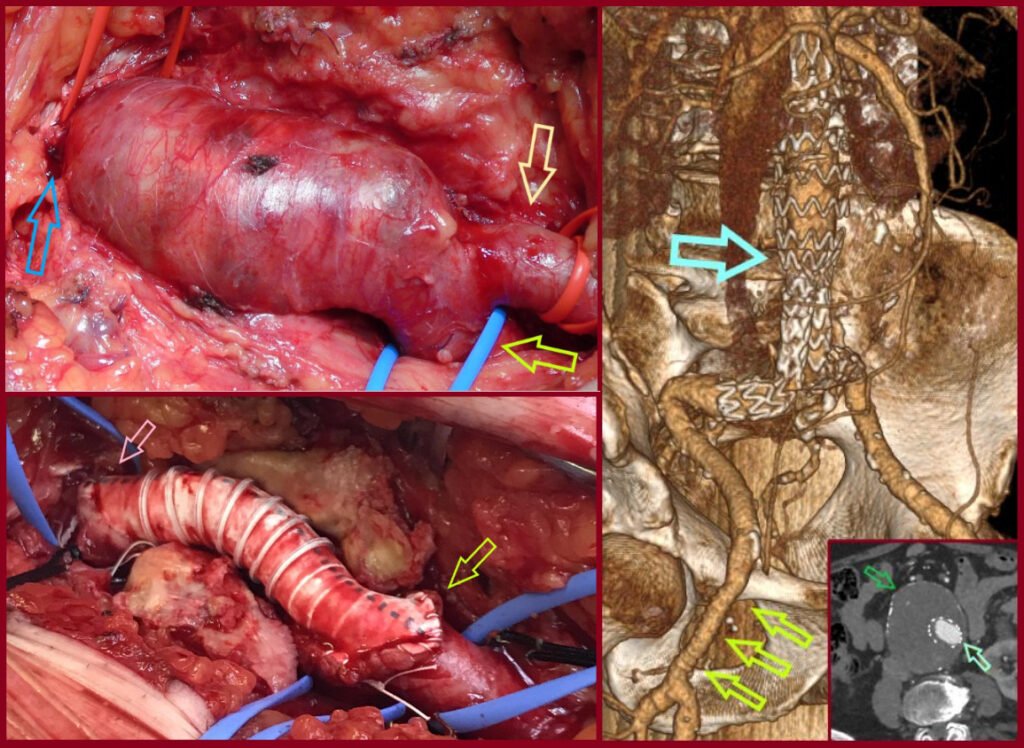
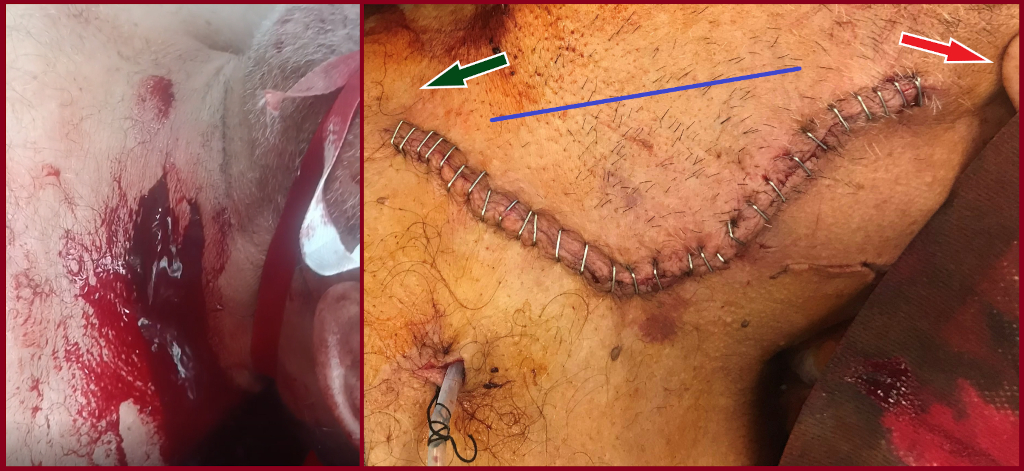
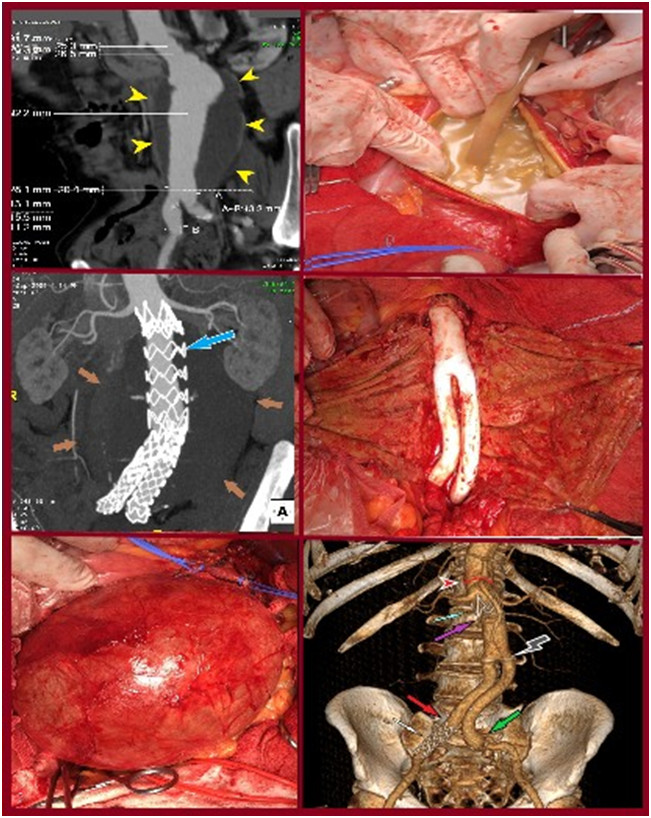
A 59-year-old-male transferred from a local hospital with a bleeding sinus at his left groin, controlled with external bandaging. He underwent at another hospital a femorofemoral bypass due to left leg claudication, five years ago, an aortobifemoral bypass 3 years ago, a graft extension of the left limb to profunda, 1 year ago, for thrombotic complications. Postoperatively, a left groin infection was treated with debridement leading to a draining sinus. Eventually, a massive bleeding occurred through this sinus, six months later. The patient transferred to our hospital and expeditiously to the operating theater after a computed tomography angiography (fig 1). The sinus was excised and a ruptured pseudoaneurysm was found. Segments of the existing thrombosed grafts were removed and the orifices of the deep profunda femoris artery were sutured from within, as they were the source of bleeding. The wound was packed with iodinated gausses and isolated with adhesive drape. The skin was sterilized again, and the patient underwent an axillary-popliteal bypass. Cultures isolated Acinetobacter baumannii. He received Daptomycin 500mg o.d. (replaced eventually with Vancomycin 1gr b.i.d due to raising creatine phosphokinase levels) and minocycline 100mg b.i.d. He had an uneventful recovery, discharged on 33rd postoperative day under ciprofloxacin 500mg b.i.d., minocycline 100mg b.i.d., rivaroxaban 20mg o.d. and acetylsalicylic acid 100 mg o.d. He remains asymptomatic, with palpable pedal pulses, 1 year later (fig 2)…..
Simultaneous Endovascular Abdominal Aortic Aneurysm Repair and Open Repair of Common Femoral Artery Aneurysm: Short Case Series and Current Review
S. Papadoulas et al. J. Clin. Med. 2025, 14, 7988. https://doi.ord/103390/jcm14227988. Department of Vascular Surgery, University of Patras Medical School, Patras, Greece
Background: Common femoral artery aneurysms are rare and are usually associated with aneurysms at other sites, mainly the aorta, iliac, popliteal, superficial femoral, and profunda femoral artery. This combination poses the challenge of synchronous repair for clinically relevant aneurysms. Although endovascular abdominal aortic aneurysm repair is the main type of treatment for abdominal aortic aneurysms nowadays, this is not true for common femoral aneurysms, where open repair remains the gold standard. These two distinct operations could be combined in a one-stage procedure when aortoiliac and common femoral aneurysms present simultaneously. This approach potentially saves time and costs, without increasing complications. Methods: A retrospective search was conducted in the Vascular Surgery Department database of a tertiary referral center for vascular surgery, covering procedures from January 2005 to May 2025. Patients were included if they had undergone simultaneous endovascular abdominal aortic aneurysm repair and open repair of a common femoral artery aneurysm. Clinical records, operative details, imaging studies, and follow-up data were reviewed. We additionally provide a literature review regarding this approach. This review additionally incorporates the current knowledge regarding the treatment of common femoral artery aneurysms. Results: Out of 668 endovascular abdominal aortic aneurysm repair procedures, three patients (0.45%) were identified. These three patients were among five patients who were treated for true common femoral artery aneurysm by open repair in the same time interval. All of the patients are currently in good condition without late complications. One patient, who had not performed any follow-up imaging, was diagnosed with large aneurysms at other sites, 10 years later. Conclusions: The combined one-stage endovascular abdominal aortic repair and open repair of a common femoral artery aneurysm by interposition grafting is technically a simple approach that led to satisfactory outcomes.
Superficial venous aneurysms: a case-based review
Aliki Skandali, Spyros Papadoulas et al. Arch Med Sci Atheroscler Dis. 2025 Sep 26;10:e198-e210. doi: 10.5114/amsad/209875. PMID: 41142694; PMCID: PMC12550692. Department of Vascular Surgery, University of Patras Medical School, Patras, Greece
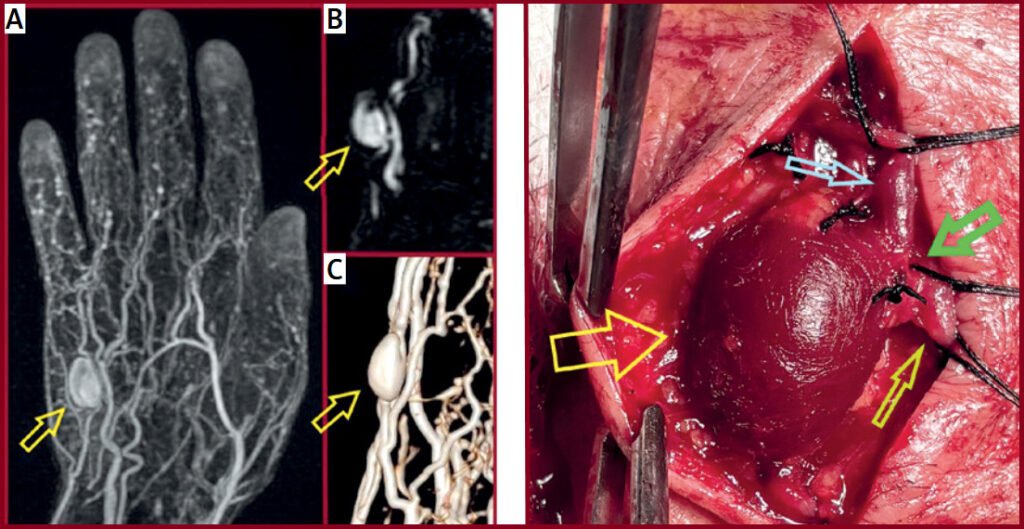
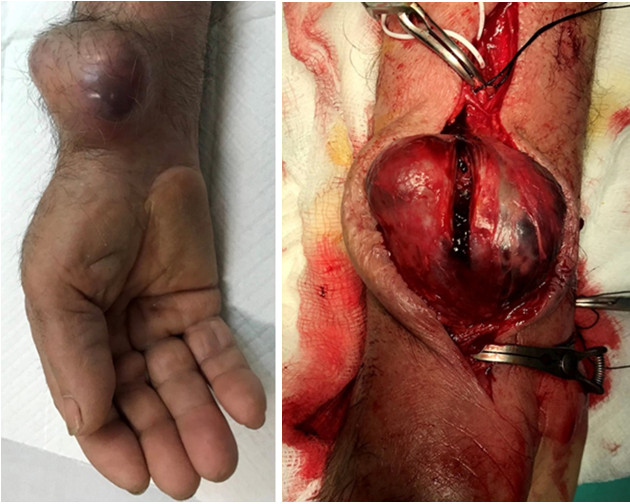
Superficial venous aneurysms and pseudoaneurysms are uncommon, frequently misdiagnosed lesions. Despite their usually benign nature, both entities can present with complications, such as thrombosis and rupture. We present a 62-year-old male patient with a superficial venous aneurysm on the dorsal aspect of his hand, successfully managed with surgical excision. Histopathology confirmed the diagnosis of a true venous aneurysm. A comprehensive literature review identified 22 superficial venous aneurysms and 9 upper extremity pseudoaneurysms. Diagnosis relies mainly on duplex ultrasonography. Currently, no standardized management guidelines exist. Surgical excision remains the preferred treatment, while sclerotherapy and endovenous ablation may be appropriate alternatives in certain cases. Heightened clinical awareness and further research are essential to developing evidence-based management strategies and optimizing therapeutic outcomes.
Penetrating internal jugular vein injury with massive bleeding
S. Papadoulas et al. Pol J Thoracic and Cardiovascular Surg 2025; 22 (2): 126-128. doi: https://doi.org/10.5114/kitp.2025.152193. Department of Vascular Surgery, University of Patras Medical School, Patras, Greece
Spontaneous avulsion of the inferior mesenteric artery in a neurofibromatosis type 1 patient: a case-based review
S.Papadoulas et al Arch Med Sci Atheroscler Dis 2025; 10: e48–e68 doi:https://doi.org/10.5114/amsad/205022. Department of Vascular Surgery, University of Patras Medical School, Patras, Greece
We present the case of successful endovascular abdominal aortic aneurysm repair (EVAR) in a 55-year-old male who presented with a ruptured infrarenal aortic pseudoaneurysm, formed after spontaneous avulsion of the inferior mesenteric artery. The avulsion occurred after lifting a heavy object. Although aortic endografting is not the first option in patients with hereditary disorders due to aortic friability and concerns about long-term durability, it is valuable in urgent cases due to lower morbidity and mortality, even as a bridging procedure. This policy is further supported by the fact that the alternative open reconstruction has been invariably associated with hemostasis issues and poor outcomes due to arterial fragility and inability to construct safe anastomoses. Finally, we present a current literature review regarding abdominal aortic and iliac pathology in patients with neurofibromatosis type 1 focusing on the type of the vascular lesion, method of repair and outcome.
Gluteal ischemic gangrene due to chronic aortoiliac occlusive disease
C. Pitros, S. Papadoulas et al. J Vasc Surg Cases Innov Tech 2025;11:101792. Department of Vascular Surgery, University of Patras Medical School, Patras, Greece
Gluteal gangrene rarely complicates interventional procedures such as angiographic embolization in the pelvis or may develop postoperatively after open ligation or endovascular covering or embolization of one or mainly both internal iliac arteries in abdominal aortic surgery if collateral circulation is compromised. On the other hand, gluteal gangrene as a primary manifestation of chronic aortoiliac occlusive disease is very exceptional in literature. We present a patient with atherosclerotic aortoiliac obstruction and a necrotic eschar on her left buttock treated with aortobiiliac bypass after digital subtraction angiography. Internal iliac artery revascularization, even contralaterally, is crucial for the healing of necrotic tissue in these patients.
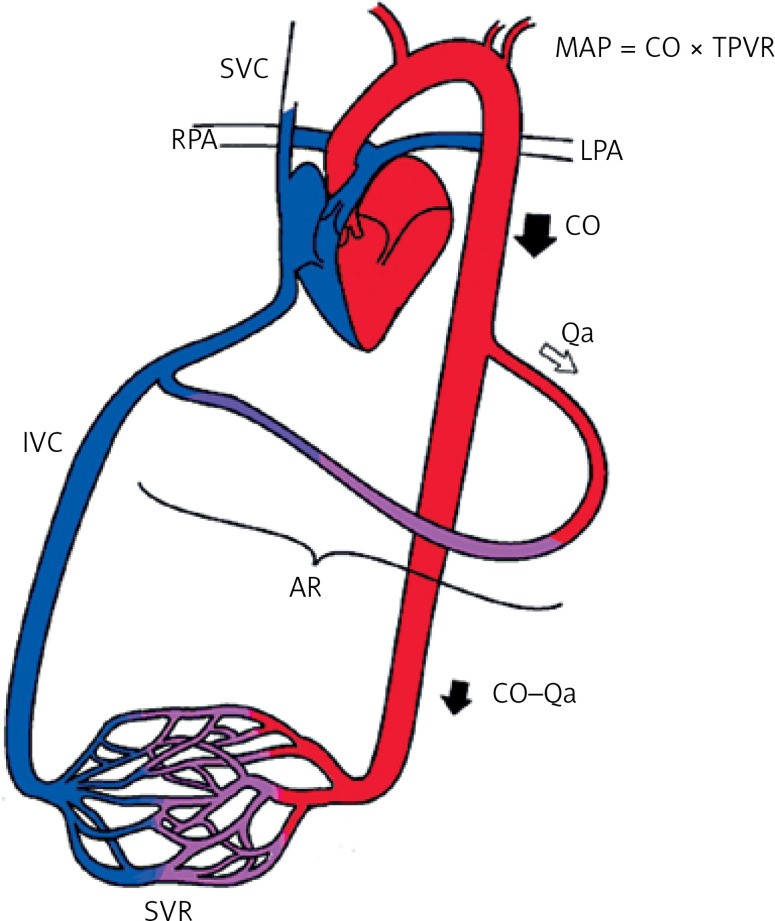
Cardiac complications of arteriovenous access: a narrative review from a multidisciplinary team perspective
Stathopoulou, S. Papadoulas et al. Arch Med Sci Atheroscler Dis 2024; 9: e217–e225. Department of Vascular Surgery, University of Patras Medical School, Patras, Greece
Although cardiovascular disease is common among hemodialysis patients, arteriovenous access creation has been invariably implicated in the evolution of adverse cardiac outcomes or deterioration of pre-existing cardiovascular disease. In most cases, these effects are subclinical but with potential underlying echocardiographic findings. Compared with grafts, arteriovenous fistulas are implicated more often, due to the progressively increased flow from the continuous dilatation of the venous outflow tract in the long term. The increasing flow is in the majority of patients well tolerated by cardiac adaptive alterations. However, the clinical impact is based on the balance between the amount of flow volume and the patient’s cardiac reserves. Having extensively reviewed the existing English literature, we present the pathophysiology and the different types of cardiovascular complications, the indications, types, and efficacy of flow-restrictive procedures in the con text of a high-flow AVF, as well as some precautions and considerations for AVF creation in high-risk patients.
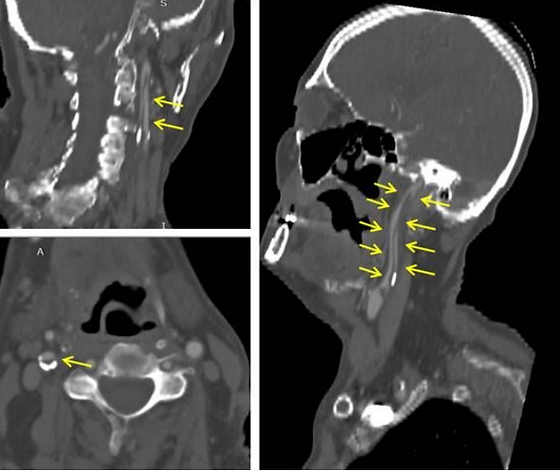
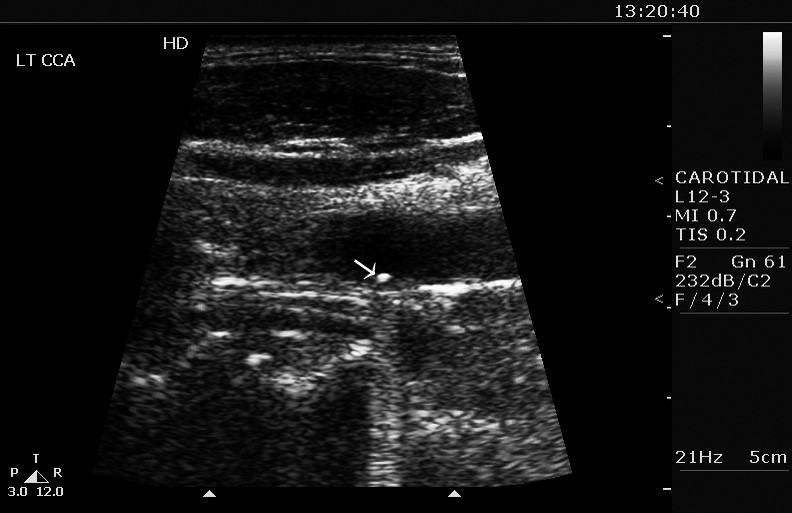
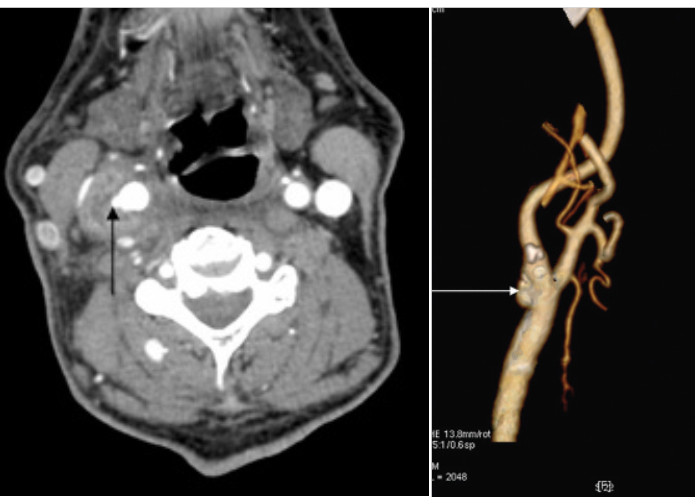
Penetrating carotid artery injury
V. Argitis, S. Papadoulas et al. Hellenic Journal of Vascular and Endovascular Surgery | Volume 6 – Issue 2 – 2024. Department of Vascular Surgery, University of Patras Medical School, Patras, Greece
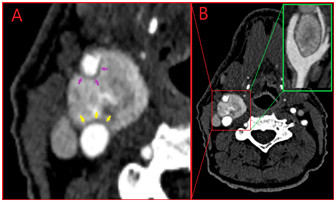
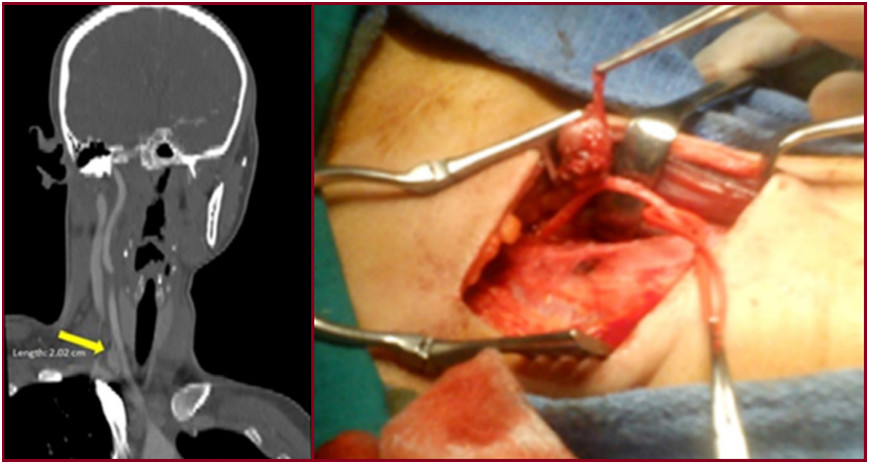
A 27-year-old male presented with a left cervical pulsative mass after penetrating trauma with a knife. No external bleeding was observed despite the presence of an open skin incision over the sternocleidomastoid muscle. Urgent Computed Tomography Angiography (CTA) revealed a partial transverse transection of the left common carotid artery (CCA) and the adjacent internal jugular vein (IJV) surrounded with a cervical hematoma due to gross extravasation from both vessels (Figure). In operating theatre, after a standard open approach for carotid endarterectomy, the CCA and IJV were clamped. The CCA was totally transected at the injury site, trimmed and re-anastomosed in an end-to-end fashion. The IJV was primarily sutured, and the hematoma was evacuated. The postoperative care was uneventful, and the patient was discharged on the 4th postoperative day. She was prescribed single antiplatelet and antibiotic treatment
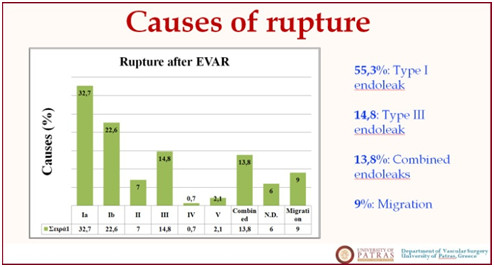
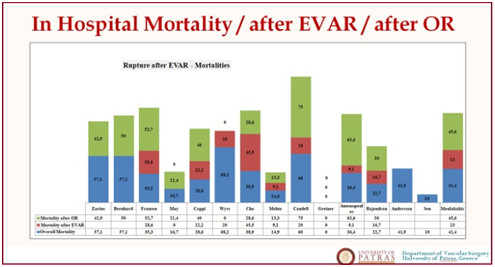
Late post-EVAR abdominal aortic aneurysm rupture: a meta-analysis study
The perivascular hypodense rim in carotid body tumor surgery
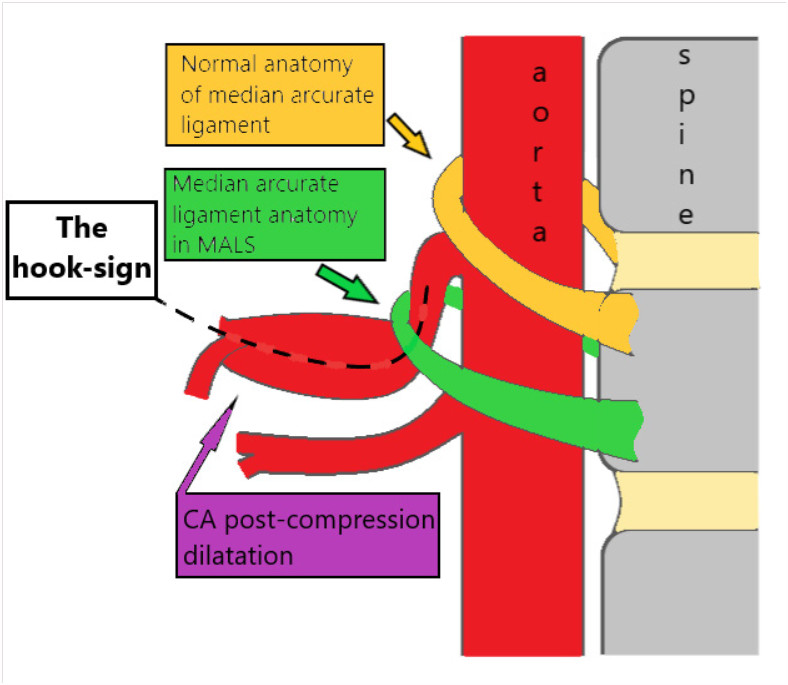
The ‘hook-sign’ in the Median Arcuate Ligament Syndrome
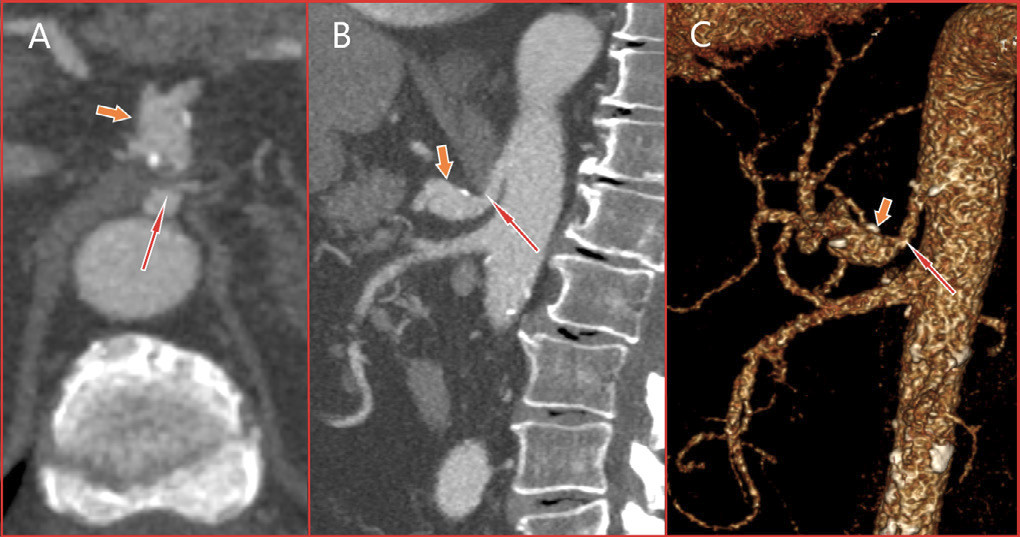
An 83-year-old male, former smoker with a medical history of hypertension and a thoracic aortic aneurysm was presented complaining of itching and edema of his legs. Symptoms were attributed to tactile skin purpura. An abdominal computed tomography (CT) scan was performed to rule out a para-neoplasmatic syndrome. An asymptomatic compression of the celiac artery by the median arcuate ligament (MAL) along with celiac artery kinking and a significant post-compression dilatation (15x15mm in size) was depicted. A following CT An-giogram (CTA) delineated the arterial anatomy and suggested the co-existence of an asymptomatic median arcuate ligament syndrome (MALS), (Figure 1). Median arcuate ligament syndrome was first described in 1917 by Lipshutz who noticed the overlapping of the artery by the diaphragmatic crura in an autopsy. It is a rare condition characterized by recurrent episodes of epigastric pain, nausea, diarrhea, and weight loss. The pain tends to be postprandial with a recession when leaning forward. Symptomatology is attributed to celiac artery compression by the arch-shaped ligament. Lower origin of the celiac artery or superior position of the MAL may predispose to MALS. The distortion of the CA centerline creates the ‘hook-sign’ (Figure 2). Sometimes, a neuropathic pain may be apparent due to ischemia or compression of the celiac ganglion. Current treatment consists of laparoscopic ligament transection followed by celiac artery angioplasty. A post-stenotic aneurysm larger than 2cm is generally
repaired by covered-stents or open surgery.
Multiple skip incisions technique for two-staged basilic vein transposition: a good alternative to the standard single long incision
A 58-year-old-male on hemodialysis underwent a two-staged tunneled basilic vein transposition with three skip incisions. Initially, preoperative color-duplex mapping was performed and a standard brachio-basilic arteriovenous fistula with the median cubital vein was accomplished. Six weeks later, after the arterialization of the basilic vein, the second stage took place after skin marking of basilic vein’s location by ultrasound. Under local anesthesia, the basilic vein and the cubital vein were dissected free from the arterial anastomosis up to the confluence with the axillary vein, using hook/right-angle retractors to dissect the vein under the skin. The vein was transected peripherally, tunneled subcutaneously in a new lateral route, after a small skin incision in the mid-upper arm, and re-anastomosed. The incisions were closed in a standard fashion. The access is still functional during the last six years. Multiple skip incisions compared to a single long incision have a better cosmetic result and cause less tissue damage. A single incision offers easier vein dissection, needs less operative time but leaves back a longer scar. Multiple skip incisions technique would have the theoretical advantage of reduced postoperative pain, oedema and surgical site infection/dehiscence rates. This is supported in some reports1 but in others, although these complications were encountered infrequently, the difference did not reach statistical significance.

Recurrence of a Resected Carotid Body Tumor Presenting as a Vagal paraganglioma
Purpose: To present a rare case of carotid body tumor recurrence presenting as a vagal paraganglioma. Vagal paragangliomas represent. Case report: An asymptomatic 25-year-old female was diagnosed with a vagal paraganglioma 3 years after an ipsilateral carotid body tumor resection. which had been fully excised as was shown by the pathology specimen examination and a recent Computed Tomography Angiography (CTA). Preoperative presumed diagnosis was based only on duplex scan and CTA. No biopsy was performed because it is contraindicated due to high vascularity of these tumors. Vagal Paraganglioma resection was easily performed because the patient was thin with a clean surgical field locating just distal to the previews operated area. Pathology specimen was conclusive for paraganglioma and his conjunction with the vagus nerve found on operation was indicative for a vagal paraganglioma. The patient remains without recurrence during the last 4 years. Conclusion: This case emphasizes the necessity of a strict postoperative follow-up protocol after resection of paragangliomas, as recurrence is always possible.
Endotension as a Rare Complication to Endovascular Abdominal Aortic Aneurysm Repair.
Papadoulas SI, et al. Innovations (Phila) 2023;18(5):498-502. doi: 10.1177/15569845231191129. Epub 2023 Aug 8. PMID: 37551670. Department of Vascular Surgery, University of Patras Medical School, Patras, Greece
Myasthenia Gravis and Abdominal Aortic Aneurysm: A Rare Combination
Abdominal aortic aneurysm in a patient with myasthenia gravis (MG) is extremely rare. We present a 64-year-old male with MG and an asymptomatic abdominal aortic aneurysm treated endovascularly. After extubation, he suffered a cardiac arrest due to an acute myocardial infarction. Cardiopulmonary resuscitation and a primary coronary angioplasty led to a satisfactory outcome. Special care is needed due to higher rates of postoperative complications in these patients.
Endovascular Repair of an Inflammatory Abdominal Aortic Aneurysm Combined with a Congenital Pelvic Kidney: Case Report and Literature Review.

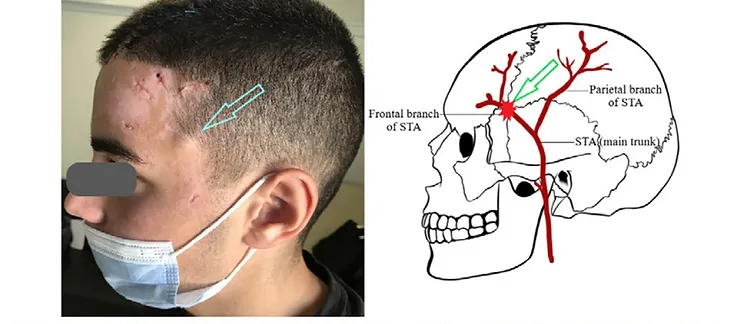
Superficial temporal artery pseudoaneurysm after blunt trauma: A case series
A case report of surgical repair of a post-catheterization radial pseudoaneurysm.
Papadoulas SI, et al. Treatment options for dialysis access steal syndrome.
Patient Transfer with Kocher Forceps on the Axillary Artery: A Rare Case of Ongoing Iatrogenic Vascular Injury.
Treatment of Dialysis Access Steal Syndrome with Concomitant Vascular Access Aneurysms

Short interposition grafting for dialysis-access steal syndrome treatment.
Papadoulas S et al. BMJ Case Rep. 2022 Feb 28;15(2):e248446. doi: 10.1136/bcr-2021-248446. Department of Vascular Surgery, University of Patras Medical School, Patras, Greece
Iatrogenic tibial arteriovenous fistula after Fogarty balloon catheter graft thrombectomy
Spyros Papadoulas et al. Clin Case Rep. 2021 Nov 9;9(11):e05050. doi: 10.1002/ccr3.5050. Department of Vascular Surgery, University of Patras Medical School, Patras, Greece

Custom-Made Bifurcated Prosthetic Graft for Aortoiliac Aneurysm Repair
Free-Floating Thrombus in the Distal Internal Carotid Artery Causing a Stroke
Adjunctive vacuum-assisted aspiration thrombectomy in a patient with acute limb ischaemia and peronea arteria magna

A Rare Case of a Small Iliac Aneurysm Causing Iliac Vein Thrombosis
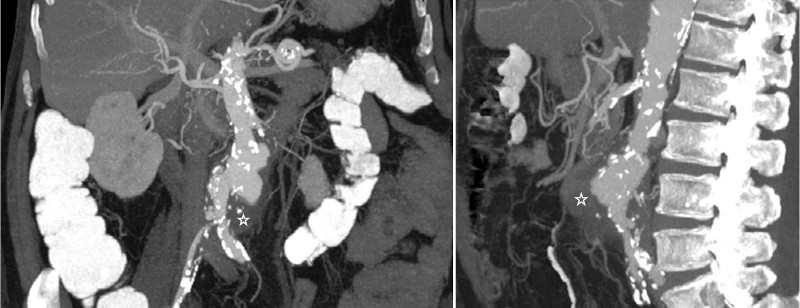
A Mycotic Saccular Aneurysm Diagnosed With 18F-Labelled Fluoro-2-Deoxyglucose Positron Emission Tomography/Computed Tomography Scanning
A Stent Graft Visualised Through an Infected Haemodialysis Graft Pseudoaneurysm
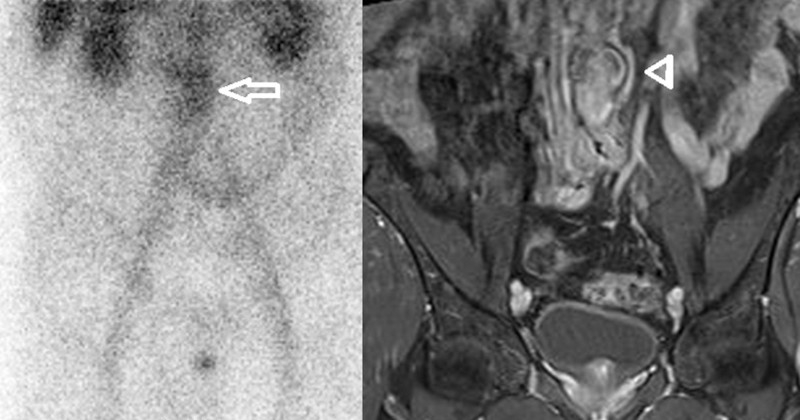
Fever of Unknown Origin due to a Mycotic Abdominal Aortic Aneurysm First Diagnosed with Bone 99mTc Scintigraphy.
Listeriosis infection of an abdominal aortic aneurysm in a diabetic patient.
Retained subintimal pellet in a carotid artery.
Mycotic aneurysm of the internal carotid artery presenting with multiple cerebral septic emboli.
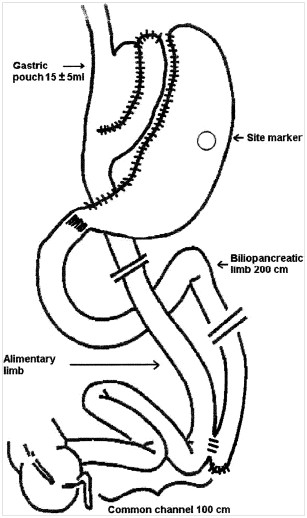
Prospective evaluation of biliopancreatic diversion with Roux-en-Y gastric bypass in the super obese.
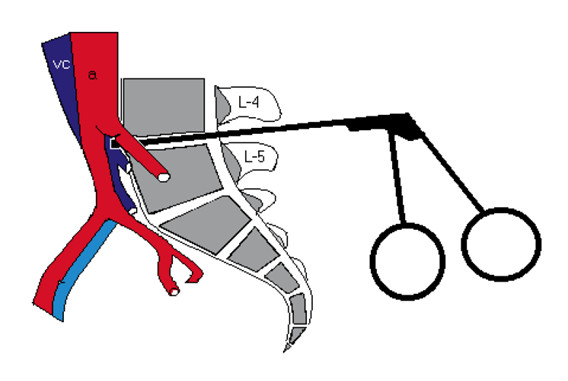
Vascular injury complicating lumbar disc surgery. A systematic review.
Ruptured aneurysms of superficial femoral artery.
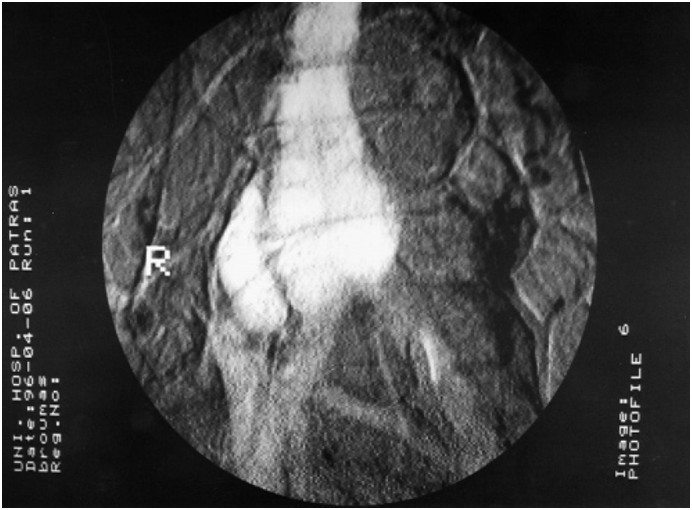
Aortocaval fistula in ruptured aneurysms.
Objectives: to study incidence, clinical presentation and problems in management of aortocaval fistula in our series.Design:retrospective study.Materials: during a seven-year period, 112 patients operated on for abdominal aortic aneurysm, including four patients with aortocaval fistula.Methods:standard repair of aortocaval fistula from inside the aneurysmal sac was the preferred operative technique.Results:the incidence of aortocaval fistula was 3.6%. Three cases were found incidentally during emergency surgery for ruptured aneurysms; the fourth case was an isolated aortocaval fistula associated with inferior vena cava thrombosis, diagnosed preoperatively by angiography. In this case, inferior vena cava ligation instead of standard aortocaval repair was performed.Conclusions: Aortocaval fistulas, although rare, should be kept in mind, because clinical diagnosis is often difficult. Furthermore, unsuspected problems during repair may necessitate appropriate change in operative technique.